-
 J. Michael Jumper, MD, Editor in Chief
J. Michael Jumper, MD, Editor in Chief
FDA Approves World's First Artificial Retina
Spring 2013
ASRS PRESIDENT JOHN T. THOMPSON, MD, COMMENDS
MARK HUMAYUN, MD, PHD, AND THE ARGUS II TEAM

Congratulations to Mark Humayun from The Doheny Eye Institute at the University of Southern California and his colleagues for taking the artificial retina from an improbable dream to reality over the past 25 years. Dr. Humayun implanted the first Argus I device in the world in 2002, and then in 2007, placed the first Argus II implant—the device that has just received FDA approval.
This work represents a scientific tour de force, as the researchers had to solve many bioengineering problems to create a functioning implant that would allow the transmission of signals from an external camera to the neurosensory retina. The chip implanted on the retina also had to be well tolerated, and the electrical signals not damage the retina with long-term use. The studies with the Argus II implant showed improved quality of life for patients with profound vision loss prior to surgery.
The Argus II milestone has important implications for many people with visual impairment. Designs of retinal prostheses will continue to evolve over the next decade as more sophisticated software is developed and more electrodes can be fitted onto the chip, allowing better visual acuity.
Retina Times Talks With Argus® II Developer
Mark Humayun, MD, PhD
On February 14, 2013, the US Food and Drug Administration (FDA) approved the Argus II Retinal Prosthesis System, the first implanted device to treat adults with advanced retinitis pigmentosa (RP). The development of a retinal implant was the brainchild of ASRS Executive Committee and Board Member Mark S. Humayun, MD, PhD, who has devoted 25 years to its research and development.
Retina Times Editor-in-Chief J. Michael Jumper, MD, spoke with Mark Humayun about the Argus II and its practical implications for ASRS members and patients.

Mark S. Humayun, MD, PhD
Associate Director of Research
Doheny Eye Institute
Cornelius Pings Professor of Biomedical Engineering
Professor of Ophthalmology, Biomedical Engineering, Cell and Neurobiology
Keck School of Medicine of USC
USC Viterbi School of Engineering
University of Southern California
Mike Jumper: Mark, who is the ideal patient for Argus II?

Figure 1: The Argus II’s video camera and transmitter are mounted on a pair of sunglasses. A video processing unit is worn on the patient’s belt.
Mark Humayun: The Argus II is FDA approved for patients age 25 and older with advanced RP. It is intended for patients with bare light perception or worse vision due to retinitis pigmentosa.
Argus II patients cannot have other diseases that damage the optic nerve like glaucoma, nor currently use anti-glaucoma drops, nor have a history of retinal detachments. It doesn’t matter if they have cataracts or an intraocular lens; most patients in the study had those.
Mike Jumper: How many patients could the Argus II be useful for in the United States?
Mark Humayun: The Argus II is approved as a humanitarian-use device, so it’s for an orphan indication; this is because even though RP has an incidence of about 1 in 4000, the number of patients who end up with this severe loss is smaller—there are probably 10,000 such patients today, with an annual incidence of a few hundred patients. That’s whom it’s planned for initially.
Mike Jumper: What do you tell prospective Argus II patients they can expect?
Mark Humayun: I make sure that patients who meet the criteria clearly understand that Argus II involves not only surgery, but a post-operative programming and low-vision rehabilitation protocol. Patients will need to return periodically to get the software and the electronics customized to their needs and to begin using this device. Many have been blind and have not had useful vision for decades so, with an occupational or low-vision therapist, they have to relearn to see.
After going over the surgical risks and benefits, it’s important to explain this rehabilitation period—something that’s common for orthopedic surgeons, but not for us as ophthalmologists and retina specialists. Beyond that, I give patients a reasonable expectation of what they should be able to get from this device, and talk about what other patients have been able to do.
Mike Jumper: What level of vision can Argus II patients expect to achieve?
Mark Humayun: In the study, independent observers evaluated a host of activities of daily living. Being able to distinguish light from dark, and identify doorways and curbs and even alphabetic characters, are the ones that make the headlines, but there are a number of other things. Laundry sorting—being able to identify and sort black, gray, and white socks—was one such objective.
Argus II helps improve orientation and mobility; it tells you where the large objects are, where the windows and doors are, and allows you to see sidewalks and curb sides. It helps you to see people, determine where they are, and see how they are moving. It then allows you to do certain chores like sorting laundry. Those are the kinds of things that are reasonable to discuss with any patient thinking about getting this implant.
Mike Jumper: Would patients be able to see burners on a stove well enough to use them?
Mark Humayun: Yes. I think they’re able to certainly see the burners and feel the heat. This sort of device adds to what patients are normally able to do. Another example is the cane. A tall patient of mine said he would get hit in the head and shoulders with tree branches and other things because the cane could tell him only what was down below. Argus II can be used in conjunction with a cane or other mobility aids that these patients are already using to get about.
Mike Jumper: If there are 10,000 advanced-RP patients right now in the US, how will these people get the device implanted?
Mark Humayun: The current plan is that most US centers that participated in the trial, along with a handful of new ones, will be implanting in 2013. Current centers are located in San Francisco, Los Angeles, Baltimore, Dallas, and Philadelphia. Second Sight Medical Products—the company that developed the Argus II, sponsored the clinical trial, and manufactures the device—is actively recruiting more centers to cover areas of the country that have no access. In all, there may be a dozen centers by the end of 2013.
In Europe, the device is approved for hand motions vision, but as you move up the ladder into count fingers and better vision, you could see that the numbers would grow and additional centers would be added.
Mike Jumper: How soon will the device be commercially available to those centers so they can start implanting it in non-study patients?
Mark Humayun: Second Sight is now working on reimbursement issues. They have several initiatives before the Centers for Medicare & Medicaid Services (CMS) and are working hard to get coding, coverage, and payment. The exact time line on reimbursement is difficult to predict. CMS could have some preliminary coverage in place later in 2013, but it could take until 2015 or longer to have full coverage and coding of the system, surgery, and therapy (including programming and rehab), along with replacement parts, in all care settings.
I understand that third-party payers are actually very receptive and are trying to help. Certainly that has been the case in several European countries.
Mike Jumper: Then you need to have a packaging plan and a way of getting the device to the centers where it will be implanted?
Mark Humayun: The device is being sold in Europe after being approved in February 2011, and Saudi Arabia has approved it. With those approvals, the Argus II has been packaged, shipped, and stored. We know about shelf life and issues like that—so that’s the good news. We don’t have to wait for those things, but we do have to wait for reimbursement details.
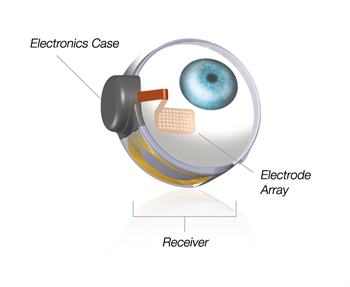
Figure 2: The retinal implant consists of a small electronics package and antenna placed around the eye under the muscles, and a 60-electrode array.
The worldwide demand is great, so the company is ramping up its manufacturing to meet it. The final assembly steps are very laborious, almost like those of a Swiss watchmaker. As they get more automated, they'll be able to fill the demand in Europe and certainly in the US as well.
Mike Jumper: So how would you counsel your patient who’s 25 years old, has RP, is the perfect candidate for Argus II, and you expect him to live another 50 years? There are going to be software upgrades that will help him better use the electrode array in his eye. But do you think this electrode array itself will need to be upgraded in the future? What’s the rate-limiting technology for the device that’s actually implanted on the surface of the retina? How rapidly will that evolve so we’ll get greater arrays and higher resolution?
Mark Humayun: I’m always asked this—will the device currently available be obsolete? Will there be a new upgrade? We’re so used to these sorts of frequent upgrades with cell phones and laptops, but the reality is that every upgrade needs to be approved by the FDA. Even software has to go through a verification and validation process. Implant upgrades are difficult and they’re a long time coming—in 4- to 6-year cycles at best, and often longer.
I tell patients the next steps that are going to make a big difference will be in the software and external hardware, and those improvements—once approved by the FDA—can be readily uploaded to their external system and require no change to the implant.
So the software and external upgrades will go a long way. Beyond that, obviously these devices are made to be removable. We have removed them from some patients, and in the preclinical studies, we had to show that we could remove them. You can put other devices in if there are future hardware upgrades, so that’s what I tell patients. But first, you have to set the expectations—this is not consumer electronics.
Mike Jumper: I understand the surgical technique for implanting the Argus II involves a pars plana approach similar to scleral buckling with vitrectomy. Could you elaborate?
Mark Humayun: Most of the steps and procedures of Argus II implantation are familiar to vitreoretinal surgeons. However, some parts are new, and the combination of surgical steps is unique and somewhat complex. We’re very familiar with isolating the muscles, doing conjunctival peritomy, and putting scleral buckles underneath muscles and around the eye.
There is a small electronics package and antenna that are all put around the eye underneath the muscles much like a scleral buckle is, so vitreoretinal surgeons feel very comfortable with that part of the procedure. However, their location on the eye needs to be very precise, and you have to be much more careful not to damage the antenna and the electronics.
After that is a pars plana vitrectomy. The next part is something new: we have to enlarge the sclerotomy, put the electrode array in, and then close the sclerotomy around the cable. Although the incision in the sclera is large to get the electrode array in—closer to 5 mm—you can close it all down to sub-2 mm. The next step is to tack the electrode array, centered on the macula, to the retina.
So the last 2 steps of putting in an electrode array through the sclera and then being able to tack it involve new techniques that retina surgeons can readily and easily learn. And you end the procedure by closing the remaining sclerotomies and then closing the conjunctiva and tenons over the electronics and scleral buckle.
This is a 19/20-gauge procedure because the sclerotomy for the tack insertion is 19-gauge, and the infusion has to be able to keep up with the enlarged sclerotomy to introduce the electrode array.
It’s good to have robust infusion too if you need it. Most people are worried about getting a hemorrhage through the choroid when you tack it, and we just haven’t seen that at all. Maybe it’s because of the anatomy of the choroid in RP patients.
From there, the critical step is to take the time to tack and make sure the array is very flat on the retina. If it’s not and you force the tack to flatten the electrode array, over time that electrode array will work against the tack and you will get lift-off of electrode.
Tacking is the most critical step—you have to make sure the electrode arrays are flat and where you want them to be in the macular area, and then tack, and not use the tack to force the array into a place where it doesn’t want to be.
Mike Jumper: You have intraoperative OCT. Is that something you use to ensure that you don’t have too much pressure?
Mark Humayun: I think the best way to tell that is if you get folding in the retina. So I really look for that. If you push it too hard, you get retinal folds around the edge of the array—then you just pull back on the tack a bit. But we spend a lot of time with any starting surgeons to be sure they understand the tacking.
Mike Jumper: For an experienced surgeon, is this a 2-hour procedure?
Mark Humayun: Yes. After a few procedures, I can complete one in just under 2 hours. For the first operation, I would obviously allow more time. The surgeons implanting in Europe commercially are doing it in around 2½ to 3 hours.
Mike Jumper: Before you put the tacks in, you’re closing down around the electrode array; you’re closing that 5 mm incision down to about 1.8 or 2 mm before you start to tack?
Mark Humayun: Yes. You have to suture the sclerotomies so there is no leakage—ie, the eye is watertight. Otherwise, the tack just won’t go through a soft eye wall.
Mike Jumper: Right, and then you’re not using any Tutoplast® or Vasculera™ over the array?
Mark Humayun: Thanks for bringing that up. Actually, we use a thin layer of pericardium over the cable of the electrode array where it comes out of the sclerotomy into the electronic can.
Mike Jumper: Where will the training for this new technique be available?
Mark Humayun: We have developed a training program which is available from Second Sight, and they also have a mock surgery setup. Typically, the training is done at the implanting center the day prior to the first case—and it takes about 1 to 2 hours.
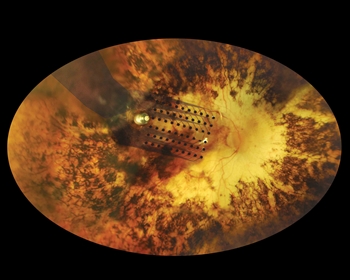
Figure 3: The Argus II’s 60-electrode array is inserted through the sclera and is tacked to the retina.
Mike Jumper: Is this something that might be offered in a wet lab, say, at the ASRS meeting?
Mark Humayun: It’s possible. The concern is, I think everybody wants to put these implants in; I’ve already had a lot of requests. But as mentioned, initially Argus II will be available at only a limited number of centers of excellence, so it doesn’t make sense to have a big wet lab and have everybody train up on it. For now, I think it’s wiser to focus on the centers that will offer Argus II in 2013 and get them up to speed.
Mike Jumper: Is the training going to be FDA mandated?
Mark Humayun: Yes. The FDA does require training of both the hospital staff and the surgeon prior to the first case. In addition to the training program from Second Sight, a surgeon experienced in Argus II implantation will be present at the first case.
Mike Jumper: What kind of rehab do you think the person who receives one of these commercial products will receive? Will there be pretty intensive rehab for weeks or months? How do you see it happening?
Mark Humayun: Rehab time has lessened considerably. Until we figured out the kind of software code needed and how to rehab patients, the process took a long time; it took 2½ years to get the first patient to a certain level of vision. In the latest patients in Europe, it's taken about 2 months.
Today, rehab is typically performed after the device has been programmed, and most patients go through a rehab program that involves 10 to 15 sessions of about 1 hour each. These sessions tend to be spread out over the first 3 months post-operatively. The occupational or low-vision therapist works with the patient to teach basic skills, identify important goals, and help the patient achieve them.
Mike Jumper: What is the treatment regimen after the patient completes post-op rehab?
Mark Humayun: Once a patient finishes post-op rehab, the sessions are once quarterly. Patients do get their settings looked at, and of course we want to look at the patients once quarterly as well. This is not an implant you put in and then forget about it; you do need to follow the patients periodically.
Mike Jumper: So is this like a model for pacemakers or cochlear implants, where the company will employ engineers for field support?
Mark Humayun: In the early days post-launch, the company will provide extensive field support. And there will always be a place for field services provided by the company for difficult or unusual cases. But as with the cochlear implant, independent specialists likely will be trained to program the devices, just as audiologists do for cochlear implants.
Mike Jumper: Now that the Argus II is FDA approved for RP, how soon do you think it might be approved for treating other conditions such as AMD?
Mark Humayun: The device in its current format is approved only for patients with light perception or worse vision due to outer retinal degenerations; this is not the level of vision loss experienced by patients with macular degeneration.
The amount of acuity that needs to be provided for macular degeneration patients depends on the stage of the disease and patient expectations. It is not yet clear whether there needs to be an evolution in the technology to treat these patients. Second Sight hopes to address this open question by running a small pilot study in the most severely affected AMD patients to see if the Argus II provides any benefit.
Mike Jumper: What enhancements are being studied?
Mark Humayun: We are exploring image-processing techniques such as zoom and finding that some patients with the Argus II are able to achieve 20/200 acuity. That’s a big jump from 20/1260 without zoom.
Envision, for example, that when you’re sitting at a table to see something fine, you can zoom in, and then when you’re walking, you can zoom back down to zero magnification. Those sorts of schemes will definitely come into play.
Mike Jumper: Other than RP and AMD, are there more retinal conditions you’re looking to treat with Argus II technology?
Mark Humayun: We’re looking at conditions with photoreceptor loss, namely outer-retinal degeneration—anything that damages the outer retina. Could we use it in patients with retinal detachment? That’s the one that everyone asks me about—“Yeah, we fixed this person’s retina and it’s attached, but he doesn't see very much.” I don’t know whether the Argus II could help those patients, but in some cases it might be worth exploring.
Mike Jumper: What made you decide to pursue retina research?
Mark Humayun: I wasn’t going to be an ophthalmologist, but then my grandmother developed diabetic retinopathy. This was in the late 1970s and early 1980s when we were just starting to understand the role of laser, and those diabetic retinopathy studies were ongoing. I took her to all the leading places, and they were contemplating what to do and what not to do.
My grandmother ended up going blind in both eyes from diabetes; it made me rethink my career path and pursue ophthalmology and a PhD in biomedical engineering. If it hadn’t been for her, I wouldn’t have been an ophthalmologist or a biomedical engineer and certainly would not have pursued this field.
I am fortunate to have been helped by many along the way, and especially Second Sight Medical Products, as without a dedicated company focused on developing such an implant, it would have remained a research project.
Mike Jumper: Mark, has this research followed the time line you expected?
Mark Humayun: I’ve been working on it since 1987. In 1992, we tested some electrodes in a patient. Once we put electrodes in a blind person’s eye and that person could see the electrical stimulation—even though it wasn’t implanted—things got heated up and people had a lot more interest.
It’s been a rollercoaster in many ways—up and down for the last 25 years. Many nights you think it’s not going to work, and other days it’s pure joy because you think you got it—only to find there have many more turns in the road. You just can’t predict this kind of research. It’s a good thing I just enjoyed it all along the way.
Mike Jumper: Yes. You liked the road you were on, lengthy as it was.
Mark Humayun: You have to enjoy the road you’re on; otherwise, these sorts of projects can end up being too taxing. Could I have done it faster? No. We didn’t know the information. I think we needed the 25 years to develop it.

Argus II Development? Think Decades, Not Years
An ASRS colleague recalls the early days of artifical-retina research
I had the pleasure of meeting Mark Humayun in 1990 at the 21st Annual Neural Prosthesis Workshop at the National Institutes of Health. Our posters describing the concept of developing a retinal prosthetic were placed side by side. At the time, I thought no one had ever presented such an idea—though I later learned that Mark and his colleagues had first presented their concept for an artificial retina at the 1988 ARVO meeting.
Earlier attempts by others to create a visual prosthetic by applying electrodes to the visual cortex had largely failed.
October 1990[1]
By 1990, scientists were beginning to learn more about chronically stimulating neurons without killing them and how to design electrodes that would not degrade in the process. Ophthalmologists, by then comfortable with vitrectomy, could access the retinal surface and the subretinal space. The time was right for creation of a retinal prosthetic.
At the workshop, Mark Humayun was a graduate student in biomedical engineering at the University of North Carolina and an ophthalmology resident at Duke University. He had already been working on this project since 1987, and engineers were designing the earliest prototype. I was a retina fellow at the Jules Stein Eye Institute at UCLA. As a resident, I had also developed the idea of creating a subretinal or epiretinal prosthetic. My colleagues and professors considered my idea eccentric. (I think they actually thought I was nuts!)
October 1990[2]
When I met Mark, I felt vindicated that not only did someone else have a similar, wacky idea, but that others felt it was worth pursuing. I knew that bringing this idea to fruition would require an enormous amount of dedication—and that is exactly what Mark Humayun has provided.
He has doggedly pursued this retinal prosthesis concept over the past 25 years as a graduate student, ophthalmology resident, retina fellow, and professor. I watched him from a distance with pride (and envy) as the prosthesis developed. For years, the “proof of concept” was still elusive. Now, almost 23 years after meeting Mark Humayun, he has my admiration and I offer him my heartfelt congratulations.
References
1. Humayun MS, de Juan Jr E, Sato Y, Propst R, Timmins M, Venkatasubramarian R, Phillips H; Duke Eye Center. Intraocular Retinal Microstimulator [poster]. Presented at: National Institutes of Health 21st Annual Neural Prosthesis Workshop, October 17-19, 1990, Bethesda, MD.
2. Foxman BT; Jules Stein Eye Institute. Rationale for the Development of an Intraocular Visual Prosthesis [poster]. Presented at: National Institutes of Health 21st Annual Neural Prosthesis Workshop, October 17-19, 1990, Bethesda, MD.
Financial disclosures
Dr. Jumper – COVALENT MEDICAL, INC: Equity Owner, Stock; DUTCH OPHTHALMIC USA: Speaker, Honoraria.
Dr. Humayun – SECOND SIGHT MEDICAL PRODUCTS, INC: Consultant, Investigator, Intellectual Property Rights, Stock.