Retinopathy of Prematurity
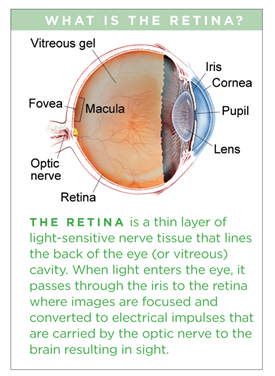
Retinopathy of prematurity (ROP) is a condition affecting premature infants of low birthweight (BW) and young gestational age (GA). It occurs when the development of normal retinal blood vessels, which typically requires a full-term pregnancy for completion, is interrupted by the premature birth. If the disease progresses, scar tissue can grow; this can lead to retinal detachment and vision loss.
Though great strides have been made in the care of profoundly premature infants and survival rates have improved considerably, ROP remains a leading cause of lifelong visual impairment. ROP causes visual loss in 1300 children and severe visual impairment in another 500 children each year in the United States alone.
More mildly affected infants may experience moderate vision loss and crossed eyes.
Symptoms
In 85% to 90% of cases, ROP of milder severity resolves on its own, with no meaningful impact on vision. If ROP progresses to an advanced stage, an infant may:
- Not respond appropriately to light
- Have white scar tissue visible in the pupils
- Develop an oscillating (back and forth) involuntary eye movement (nystagmus, pronounced nis TAG mus) by as early as 3 months after the original scheduled date of birth
- Progress to blindness
Causes
The earliest cases of ROP were thought to be the result of introducing oxygen therapy into the newborn nursery to improve the survival rates of premature infants. Though more premature infants survived, some progressed to blindness. In 1942, oxygen was identified as an agent that could aggravate this process and lead to retinal detachment. Today, the use of oxygen is closely monitored and is no longer implicated as the sole or even a primary factor in ROP development. While the survival rate for high-risk newborn infants has improved, the incidence of ROP has remained constant since the mid-1990s.
Risk factors
ROP is a disease of the smallest and the sickest infants. Premature birth and low birthweight are the primary risk factors. Other risk factors for the development of ROP include:
- Multiple births
- Other health problems involving the lungs and intestines
- Infection
Diagnostic testing
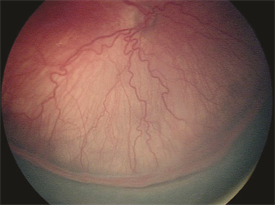
Figure 1.
Infants of low birthweight (under 1500 grams or 3.3 lbs.) and gestational age (30 weeks or less)—as well as infants deemed higher risk by the neonatologist (due to multiple births, oxygen exposure after birth, etc.)— are screened with either bedside eye exams or digital pictures of the back of the eye (retina), which are then reviewed by a physician experienced in the diagnosis and treatment of ROP. Once ROP progresses to a certain level of severity (Figure 1), treatment is recommended. Treatment is most often required between 34 to 38 weeks of gestation.
Treatment and prognosis
Since the early 1990s, ROP has been successfully treated in most infants by placing laser burns in the part of the retina that has not developed normal blood vessels. This approach prevents retinal detachment in 90% of treated eyes with few long-term side effects. Since 2007, injection of certain drugs (bevacizumab [Avastin®] or ranibizumab [Lucentis®]) into the eye to suppress growth of the abnormal blood vessels has been employed by some physicians.
To date, dosing and long-term safety information are lacking, and laser is generally the preferred approach to managing ROP requiring treatment, except for those very small babies with very aggressive ROP. If an eye goes on to develop retinal detachment, surgery may be performed to help reattach the retina, but the goal is to try to screen in order to treat ROP at the right time to stop the progression to retinal detachment.