Familial Exudative Vitreoretinopathy
(FEVR) is a hereditary condition where the retinal blood vessels do not develop normally. As a result, scar tissue may develop which—as it contracts—can detach the retina and result in visual loss.
Vision loss may also occur as a result of abnormal leaking blood vessels (exudation), and a progressive shutdown of the finest blood vessels in the eye (capillary dropout) critical for the delivery of oxygen to the retinal cells.
FEVR does not always result in vision loss, and carriers of the disease may have no visual symptoms—only to be diagnosed when there is an affected family member. Wide-field fluorescein angiography (a photographic test using an intravenous dye to provide detailed information about the structure and function of retinal blood vessels) is critical for the diagnosis and management of FEVR.
Symptoms
Vision loss is the most common FEVR-related symptom. In mildly to moderately affected individuals, crossed eyes (strabismus) and “lazy eye” (amblyopia) are often encountered.
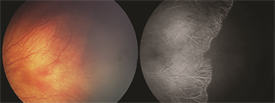
Figure 1.
FEVR is categorized in stages based on findings drawn from both the clinical exam and fluorescein angiography. In Stage 1 FEVR, blood vessels which supply the peripheral retina (the area near the retina’s edges) are “pruned,” and have a number of other abnormalities of structure and function (Figure 1). Growth of abnormal new blood vessels (neovascularization) is seen in Stage 2 FEVR (Figure 2). In Stages 3, 4 and 5 (Figure 3) the retina is detached as neovascularization contracts and puts traction on the retina.
Causes
FEVR develops as a consequence of a genetic abnormality (Wnt signaling) that affects growth and development of retinal blood vessels. Apart from heredity, there are no specific risk factors.
Diagnostic testing
Diagnosis of FEVR may be challenging due to the overlap in findings with other pediatric conditions characterized by abnormal development of retinal blood vessels.
Strategies to help with diagnosis include:
- Evaluation of the fellow eye by both direct examination and wide-field fluorescein angiography, since FEVR typically affects both eyes, although often not to the same degree
- Examination and fluorescein angiography of family members, as up to 90% of the time an affected asymptomatic family members will have clinical or angiographic findings
- Genetic testing (FZD4, NDP, TSPAN12, and LRP5) (This confirms the diagnosis in approximately half of patients with FEVR.)
Treatment and prognosis
Early or mild FEVR (Stage 1, Figure 1) without leaking blood vessels (exudation) is generally managed by observation without treatment. If there is blood vessel leakage in Stage 2 FEVR (Figure 2) or higher, laser treatment of areas of the retina without normal blood vessels is recommended.
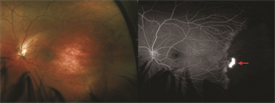
Figure 2. |
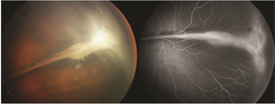
Figure 3. |
For more advanced stages 3, 4 (Figure 3), and 5, surgery can be performed to remove or interrupt scar tissue and release traction. This encourages reattachment of the retina, which can stabilize or improve vision
Once stable, individuals with FEVR are usually followed every 6 months with examination and fluorescein angiography—more often if the disease is active. FEVR is a lifelong disease. Reactivation can occur at any time.